Flaws in the 'Bad Batches' Theory
...and the search for a better explanation


This is the first article of a three-part series. Please find the other articles here:
Flaws in the 'Bad Batches' Theory (this one)
The real Story behind the Bad Covid Batches (to come)
Abstract
Having analyzed the adverse event reports of Covid-19 vaccines provided by the US American system VAERS, I confirmed the well-known observation, that more than 95% of the reported severe adverse events are related to less than 5% of the batches of all vaccine producers. But in contrast to some people who are claiming, that each of the producers, Pfizer/BioNTech, Moderna, and Janssen, had extreme variations in batch quality (poor manufacturing practices) or recipe (premeditated experiments), I have different findings.
But first, in this article, I will show evidence against the popular Bad Batch theory and a theory of largely different batch sizes. In the second article, I will examine factors that influence if an adverse event report is filed. In the final article, I will present a better explanation for the observations that caused the Bad Batch Theory, provide evidence for it, and have to draw conclusions that are much more severe.
Definitions
First, let me give some definitions to avoid misunderstandings of my statements, like the difference between an adverse event and a side effect and the different types of adverse events that I have found.
Adverse Event: "Any untoward medical occurrence that may present during treatment with a pharmaceutical product but which does not necessarily have a causal relationship with this treatment." [International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use.]
Side Effect: A peripheral or secondary effect, especially an undesirable secondary effect of a drug or therapy. [Medical Dictionary]
Serious Adverse Event: Death, life-threatening events, hospitalization, disability or permanent damage, Congenital anomaly, birth defect or abortion
Administration Error: Thousands of reports only refer to vaccine storage or administration errors without resulting in health issues, like overdose, underdose, wrong diluent and more. They are left out for a correct counting of adverse events.
Vaccination Breakthrough: Any report of a positive Covid test after Covid vaccination. Since I focus on → Real Adverse Events (see below), I ignore how soon after vaccination the breakthrough occurred.
Real Adverse Event: A VAERS report which is not related to a → Vaccination Breakthrough and is not a pure vaccine → Administration Error.
Invalid Event: The CDC checks VAERS reports and, in cases of doubt, marks a report as invalid. These were ignored in the analysis.
Observation A: Report Concentration
Using the service CDC WONDER, any internet user can perform data queries on the VAERS website, like searching Covid vaccine-related adverse event reports and create statistics, like which vaccine batches have caused adverse events. This exhibits that more than 95% of all severe adverse events were reported for less than 5% of the batches. A review of the batch codes unveils that the VAERS reports contain thousands of misreads, typos, and additional texts, but I filtered and cleaned up this data to a final list of 8,088 batch codes which are valid.
Here is a diagram of the number of severe adverse events reported per batch. Each vertical bar represents a vaccine batch and the length of the bar is the number of adverse events reported for that batch. The bars are ordered in descending number of adverse events:

On the top end of the batch list (which I call “most reported batches”), there are 198 batches with more than 1,000 reports each, but most batches have almost no reports at all.
How could this happen? Different factors have an influence on the number of reports filed for a batch:
Batch Size: If a batch contains a larger number of vaccine doses, it is normal to cause a larger number of adverse events. This is a good case in which every participant behaves as expected.
Batch Quality: If a batch has worse quality, due to errors or dosage experiments, it may cause a larger number of adverse events. This is a bad case in which manufacturers may have acted in a negligent or even illegal manner.
Reporting Quality: Not every adverse event is reported, there is a large underreporting factor. If a large part of a batch is administered to or by people that are more prone to report adverse events, then this batch will cause a larger number of reports. This is a poor case in which the reporting system does not work as expected.
By keeping two of the above factors constant and allowing one to vary, one can articulate the following three theories:
Theory 1: “Bad Batches”: Strong diversity in batch recipes or quality, similar batch size, and reporting levels
Theory 2: “Giga Batches”: Strongly different batch sizes, similar quality, and reporting
Theory 3: “Report Clusters”: Strongly different reporting levels for different batches, similar batch quality, and size
Combinations are possible too, in which two or all three factors vary. But first, let us try to find out if one of the theories above could be true. In the following text, I will describe these theories in more detail, derive expectations, check them with data analyses (observations), and draw conclusions, which theories are confirmed or falsified by the observations. Now, let me show you the second observation which has led to the Bad Batches Theory:
Observation B: Severity Pyramid
Let us check if there could be a relation of the batch code to the number of reported severe adverse events. Each square represents a batch, they are ordered alphabetically by their batch code from left to right, and the vertical position reflects the number of severe adverse events reported for that batch. The three Covid-19 vaccines admitted in the USA result in the following diagrams. What seems to be a thick smeared line on the bottom of each diagram, is the fusion of many squares for the 95% of batches with low numbers of severe adverse events:

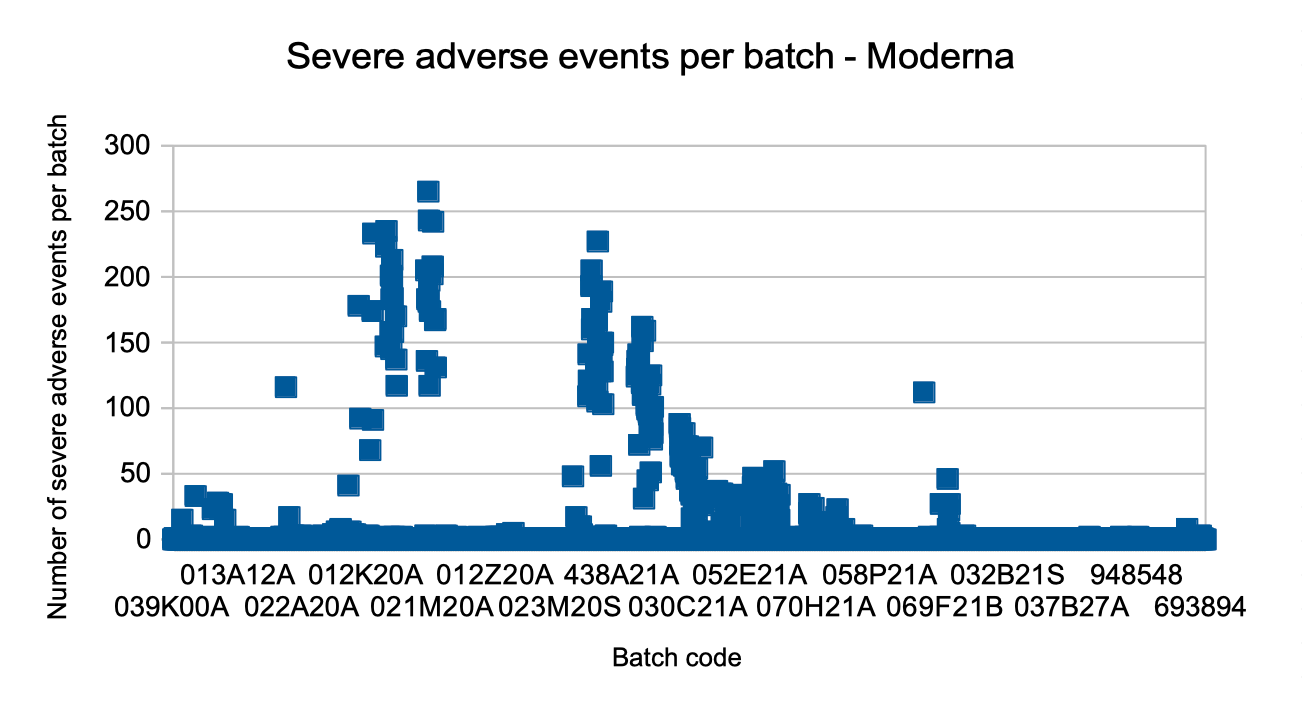

For some, at least the diagrams for Pfizer/BioNTech and Moderna looked too structured to be random, so they did further analyses and stated the following theory:
Theory 1: Bad Batches Theory
Mike Yeadon and Craig Pardekooper suspected that either the recipe or the quality of batches differs. They even stated that each batch had its distinct toxicity which was reflected in the batch code. Finally, they considered this as evidence for premeditated and unapproved dosing experiments on the population.
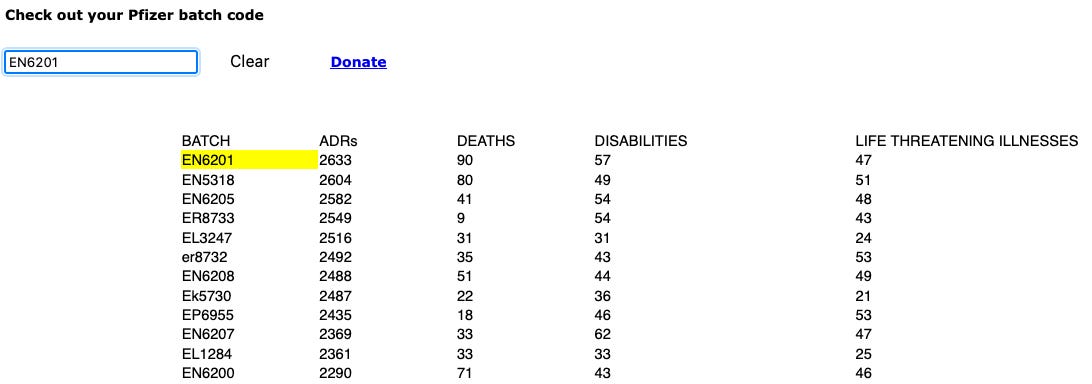
In consequence, a website How Bad is My Batch was created, offering each visitor to check the batch code of the vaccine dose he/she is going to receive in order to avoid toxic batches.
I verified these findings and went down that rabbit hole too. But with my own analyses, I came out at a different spot which I will explain in this article series.
Theory 2: Giga Batches
If each batch has the same properties but batches have different sizes, it is expected that the number of reported adverse events is proportional to the batch size. Thus, a batch that has twice the number of vaccine doses as another batch is expected to cause twice as many adverse event reports.
Since some batches must be extremely larger than the majority in order to explain the observations, I am using the term Giga Batches.
Unfortunately, the manufacturers do not disclose the sizes of their batches. It is estimated that a standard batch has a size of 300,000 to 900,000 doses.
Theory 3 Report Clusters
It is valid to assume similar consistency and quality of different batches since vaccine manufacturers are strongly regulated. A vaccine's marketing admission is granted only for a fixed recipe, which has been tested in clinical trials. Changes in the recipe or significant variations of doses are considered to be falsifications and are punished, no matter if premeditated or caused by production issues.
If, in addition, batches have similar sizes, another factor must influence the number of adverse events.
One very obvious but generally neglected factor is the difference between the occurrence and the reporting of an adverse event. Many studies have examined underreporting rates of VAERS and estimate factors of at least 5, many around 40, some even up to 100. This means, only 1–20% of all adverse events that occur, actually get reported to VAERS. If there is a factor that causes this rate to increase for one batch, for example from 1% to 8%, this batch will get 8 times more reports than the other batches, in spite of having the same size and the same ingredients.
Could this happen? I think so and will show evidence in article 3 of this series.
Observation C: Vast Microreporting
On the lower end of the batch list (“least reported batches”), there are 4,750 batches for which only one single event is reported, that is 59% of all reported batches! There were less than 8 reports for 90% of all the batches. The following diagram displays the number of events in a batch horizontally and the number of batches that have that number of reports vertically:

This is a tough observation for all the theories:
If the Giga Batch Theory was right, we can assume that the batches which cause only 1 to 7 reports reflect the standard size, making up 90% of all batches and having an average number of 1.7 adverse events per batch. But the most reported batches caused more than 5,000 reports. In consequence, these batches would need to be 3,000 times larger to cause this number of reports. This does not make sense economically and does not seem meaningful or feasible in production. I consider this evidence against the Giga Batches Theory.
Interpreted according to the Bad Batch Theory, the average number of 1.7 adverse events per batch for 90% of the batches must be considered to be the baseline for a safe and effective vaccine batch. A larger number of adverse events for a batch is supposed to be the effect of its larger toxicity. This means, that the most reported batches with 5,000 adverse event reports must have toxicity that is 3,000 times larger than the one of the baseline. It would be such an extreme overdose compared to the functioning baseline, that it does not make sense for medical evaluations. On the other hand, good manufacturing principles oblige companies to extremely high and consistent levels of product quality that 200 batches of disastrous quality hardly could ever occur. In my opinion, this is evidence against the Bad Batches Theory.
If the Report Cluster Theory is right, this would mean that for each one out of several thousand batches, thousands of adverse events were not reported and only the top 5% of batches had an appropriate level of reporting.
Observation D: Breakthrough Symmetry
VAERS provides information about vaccination breakthroughs, so let's do a thought experiment. Assuming, that the bad batches theory is right, we could make different observations:
If the 95% of “harmless” batches were placebo batches (eg. physiological salt solution) that do not cause harm, these batches would have very few real adverse event reports but hundreds or thousands of vaccination breakthrough reports.
If the “bad” batches had very high concentrations of agents, resulting in a higher immunization effect, the batches with a large number of adverse events should have few to no breakthrough reports.
A combination of the above is possible
In the following diagram, I display each batch as a column, ordered by descending number of severe real adverse events. Vertically, its number of severe real adverse events is charted in blue, and its number of breakthrough cases is on top in orange. I limited the diagram to the 524 batches with at least 3 reports of the displayed types.

Obviously, the expectations are not met: All the batches with a large number of reported severe adverse events also have a large number of breakthroughs. The presumably “weak” batches have almost no breakthroughs at all.
For me, this is striking evidence against the Bad Batches Theory. The most logical explanation for this observation seems to be the Giga Batch Theory, but also the Report Cluster Theory could apply: There are few batches which have found especially much attention: In reporting real adverse events as well as vaccination breakthroughs.
Observation E: Breakthrough Pyramid
In the last section, we have seen that breakthrough counts are approximately proportional to adverse event counts. It would be interesting to use the diagram of Observation B: Severity Pyramid to display breakthrough events!
Below, you find the severity pyramids at the left, the breakthrough pyramids at the right. In the first row, it is the data of Pfizer/BioNTech, in the second row Moderna, in the third row Janssen.


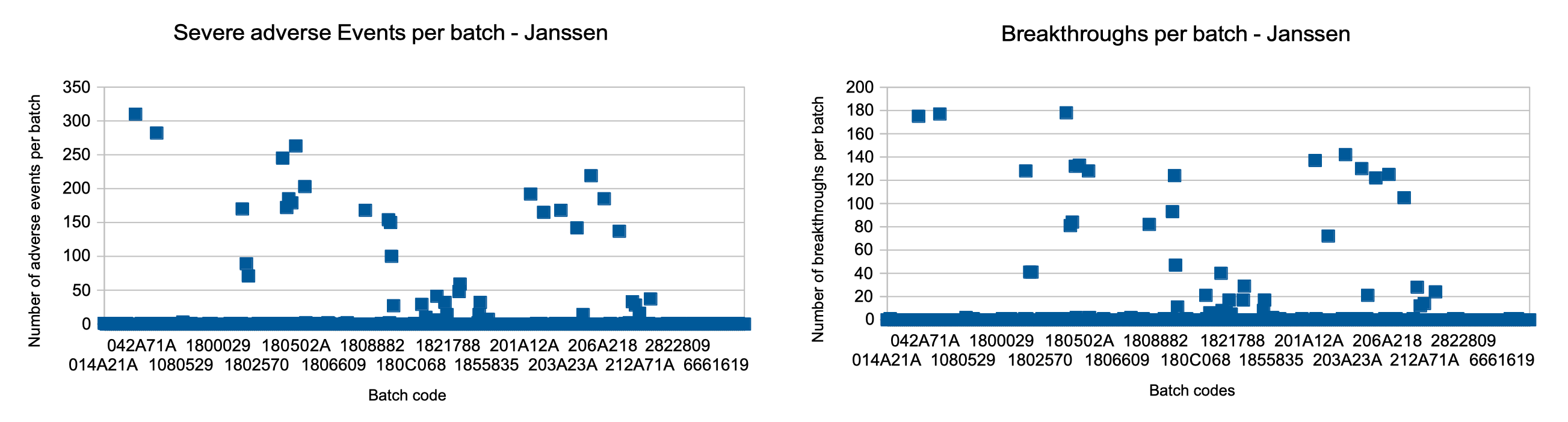
This is a tough cross-check for the Bad Batches Theory, since, it is easy to conclude premeditation for a report severity diagram because the producer controls what is inside a batch. For a breakthrough diagram, the same conclusion is absurd, since the manufacturer has no influence on infections. Recognizing very similar patterns for breakthroughs makes “Observation B: Severity Pyramid” worthless, which was the main evidence for premeditated batch toxicity. It proves that random events, outside the control of a manufacturer, can make the reporting outcome look like planned.
Observation F: No Comment
The Bad Batches Theory has found so much publicity, that the vaccine manufacturers have a vital interest to falsify these claims in order to fight vaccine hesitancy and avoid legal consequences.
For each of the manufacturers, it is a work effort of only a few minutes to check the sizes of their reported bad batches. If they would have found that the elevated report counts for their bad batches were just the consequence of the batches being significantly larger than the rest, they could have just published this information – confirming the intuitively understandable Giga Batch Theory – and the Bad Batch Theorie would have crumbled.
Well, they did not, and I value this as evidence against the Giga Batch Theory.
Observation G: Manufacturer Symmetry
As noted above, on the one hand altering a vaccine recipe after admission is a crime, and quality issues are punished as falsifications. To me it seems unlikely, that all three manufacturers act in a grossly negligent or even criminal manner. Instead, I see this as a clue that the observations are not the consequence of the producers' but of the reporters' behavior.
Observation H: Age Effect
A better explanation, of why a batch has caused more damages than another one is not found within the batch code but within the age of the vaccine recipients. A plot of all the batches with at least 10 severe real adverse events shows a clear correlation between the median age of the recipients of the batch and the resulting number of severe adverse events. Each square represents a batch, its x coordinate represents the median age of the people vaccinated with that batch, the y coordinate reflects the number of severe real adverse events reported for the batch.
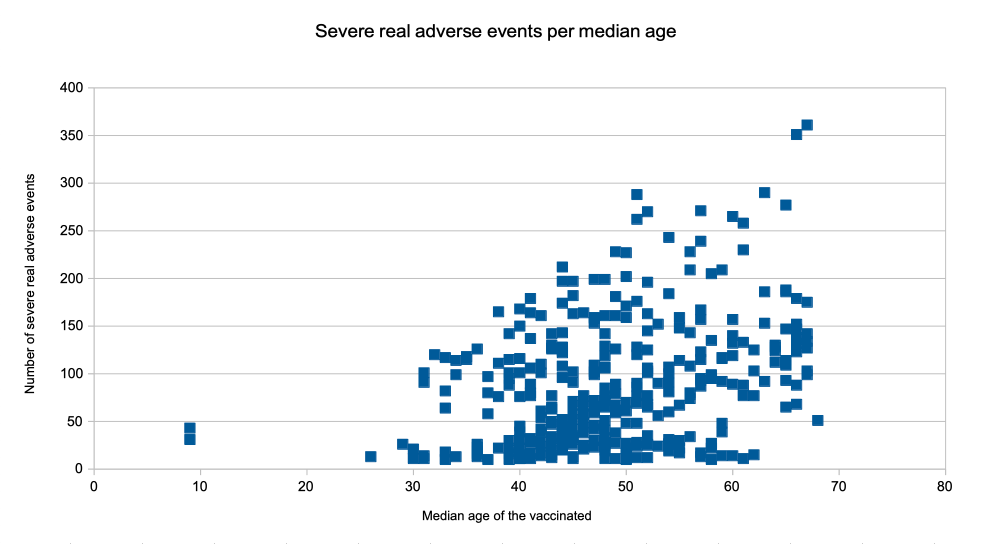
From the point of view of the Bad Batches Theory, this diagram mostly displays the Bad Batches, but it is one more observation that devalues the severity pyramid observation by showing that the age of the recipients (out of the manufacturer's control) is more important for the number of adverse events than the batch code (under manufacturer's control). So this is evidence against the premeditation aspect of the Bad Batches Theory.
For any given age group, a wide range of reports is observed. This could be the result of different causes: statistic effects, different batch sizes, different batch quality, or different reporting levels.
Conclusion
Let us sum up all theories, observations, and conclusions above:

In my opinion, this is sufficient evidence to abandon the Bad Batches Theory. Evidence against the Giga Batch Theory is rather weak, but the fact that none of the manufacturers has used it to falsify the 'Bad Batches' claims, raises suspect.
In my opinion, the Report Cluster Theory is worth a closer look which I will provide in the next two articles. Please continue reading the next article of this series “The Rocky Road to an Adverse Event Report”.
Stay tuned, stay critical, keep thinking for yourself,
Leonard Frey
(Pseudonym)
I have determined proportional reporting differences for all medical concepts in all batches.
For this one absolutely must perform age-adjustment, since different batches were distributed during different times of the vaccination campaign.
Some batches still differ in their side effects profile, but there aren't any "killer batches" out there. Well there were a couple, but I only calculated 50% confidence intervals in order not to lose to many potential signals, so some concepts are bound to be insignificantly overrepresented.
https://deepdots.substack.com/p/overview-ai-fixed-150000-lot-numbers
This guy did an excellent job on correcting mistyped batch id's.